
Statines bij patiënten met een MI en acuut hartfalen: resultaten van de EPHESUS
Literatuur - Dobre D, Rossignol P, Murin J, et al. - Eur J Heart Fail 15 februari 2013Statin therapy and clinical outcomes in myocardial infarction patients complicated by acute heart failure: insights from the EPHESUS trial.
Dobre D, Rossignol P, Murin J, et al.
Eur J Heart Fail. 2013;15(2):221-7. doi: 10.1093/eurjhf/hfs128.
Achtergrond
Bij een acuut en post-acuut myocardinfarct verbetert statinetherapie de cardiovasculaire morbiditeit en mortaliteit en mortaliteit door alle oorzaken [1-4]. Patiënten met acuut hartfalen werden echter vaak uitgesloten van onderzoek [4-8]. Statinetherapie kan ook gunstig zijn in het beginstadium van hartfalen.
In de EPHESUS studie (Eplerenone Post- Acute Myocardial Infarction Heart Failure Efficacy and Survival study)werden de effecten van de mineralocorticoïde receptor antagonist eplerenone onderzocht bij patiënten met een acuut MI dat gecompliceerd was door de klinische tekenen en symptomen van HF en linker ventrikel dysfunctie [9]. Ongeveer de helft van de patiënten gebruikte een statine bij aanvang. Deze studie onderzocht de associatie tussen statingebruik op baseline en klinische resultaten bij patiënten met acuut systolisch hartfalen opgenomen in de EPHESUS studie.
Belangrijkste resultaten
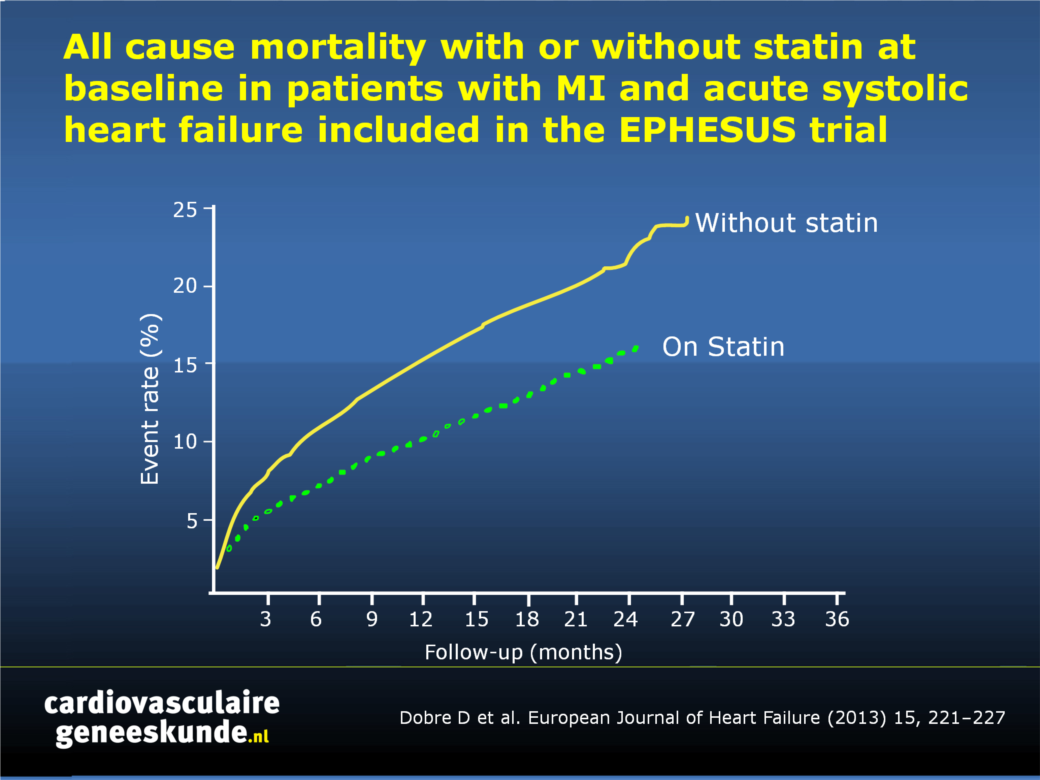
- Tijdens een gemiddelde follow-up van 16 ± 7 maanden trad sterfte door alle oorzaken op in 385 (12%) patiënten met en bij 647 (18%) patiënten zonder een statine. In univariate survival analyse was het risico van sterfte door alle oorzaken 34% lager bij statinegebruikers versus niet-gebruikers (HR 0,66, 95% CI +0.59-+0.75, P <0,001) (fig. 1).
- Na uitgebreide aanpassing bleef het risico van sterfte door alle oorzaken 20% lager bij patiënten met versus mensen zonder een statine (HR 0,80, 95% CI 0.69-+0.92, p = 0,001), vooral te wijten aan een lager risico op CV overlijden (HR 0,76, 95% CI 0,65-0,88, p = 0,0002). De vermindering van CV overlijden was voornamelijk te wijten aan een lager optreden van plotselinge dood (HR 0,77, 95% CI 0,61-0.96, p = 0,02) en sterfte door een beroerte (HR 0,53, 95% CI 0.28-0,96, P = 0,04), maar was ook te danken aan een lager percentage van sterfte door verslechtering van HF en van recidiverende acute MI.
- Statinegebruik was geassocieerd met een hoger risico van niet-cardiovasculaire ziekenhuisopnames (HR 1.16, 95% CI 1,02-1,33, p = 0,02)
Conclusie
Patiënten met acuut HF dat een acuut myocardinfarct compliceert kunnen baat hebben bij een behandeling met een statine, met een lager risico op sterfte door alle oorzaken, voornamelijk toe te schrijven aan een lager optreden van cardiovasculaire sterfte. Prospectieve klinische studies zijn nodig om deze bevindingen te valideren.Download PPT
Referenties
1. Randomised trial of cholesterol lowering in 4444 patients with coronary heart disease: the Scandinavian Simvastatin Survival Study (4S). Lancet 1994;344:1383–1389.2. Prevention of cardiovascular events and death with pravastatin in patients with coronary heart disease and a broad range of initial cholesterol levels. The Long-Term Intervention with Pravastatin in Ischaemic Disease (LIPID) Study Group. N Engl J Med 1998;339:1349–1357.
3. Heart Protection Study Collaborative Group. MRC/BHF Heart Protection Study of cholesterol lowering with simvastatin in 20,536 high-risk individuals: a randomized placebo-controlled trial. Lancet 2002;360:7–22.
4. Schwartz GG, Olsson AG, Ezekowitz MD, et al. Effects of atorvastatin on early recurrent ischemic events in acute coronary syndromes: the MIRACL study: a randomized controlled trial. JAMA 2001;285:1711–1718.
5. Cannon CP, McCabe CH, Belder R, et al. Design of the Pravastatin or Atorvastatin Evaluation and Infection Therapy (PROVE IT)-TIMI 22 trial. Am J Cardiol 2002;89:860–861.
6. Pasceri V, Patti G, Nusca A, et al. Randomized trial of atorvastatin for reduction of myocardial damage during coronary intervention:results from the ARMYDA (Atorvastatin for Reduction of Myocardial Damage during Angioplasty) study. Circulation 2004;110:674–678.
7. Patti G, Chello M, Candura D, et al. Randomized trial of atorvastatin for reduction of postoperative atrial fibrillation in patients undergoing cardiac surgery: results of the ARMYDA-3 (Atorvastatin for Reduction of MYocardial Dysrhythmia After cardiac surgery) study. Circulation 2006;114:1455–1461.
8. Pedersen TR, Faergeman O, Kastelein JJ, et al. High-dose atorvastatin vs usual-dose simvastatin for secondary prevention after myocardial infarction: the IDEAL study: a randomized controlled trial. JAMA 2005;294:2437–2445.
9. Pitt B, Remme W, Zannad F, et al. Eplerenone, a selective aldosterone blocker, in patients with left ventricular dysfunction after myocardial infarction. N Engl J Med 2003;348:1309–1321.
Abstract
Aims:Several clinical trials have shown that in patients with acute myocardial infarction (MI), statin therapy improves cardiovascular (CV) outcomes, but in these trials patients with acute heart failure (HF) were excluded or only a few were included. In patients with chronic HF, statin therapy does not reduce all-cause or CV mortality. We aimed to assess the association between statin therapy and clinical outcomes in the setting of acute HF with systolic dysfunction complicating acute MI.
Methods and results:
We performed a post-hoc analysis in 6632 patients included in the EPHESUS trial. The mean age of patients was 64 years and 71% were male. Overall, 47% of patients had a statin prescribed at baseline. Cox regression models and a secondary analysis using propensity score matching were fit to assess the association between statin prescription and clinical outcomes. During a mean follow-up of 16 ± 7 months, all-cause death occurred in 385 (12%) patients with and in 647 (18%) patients without a statin (P < 0.001). After extensive adjustment, the risk of all-cause death was 20% lower in patients on statin [hazard ratio (HR) 0.80, 95% confidence interval (CI) 0.69-0.92, P = 0.001]. This positive association was mostly due to a lower risk of CV death (HR 0.76, 95% CI 0.65-0.88, P = 0.0002). In contrast, statin use was associated with a higher risk of non-CV hospitalizations (HR 1.16, 95% CI 1.02-1.33, P = 0.02).
Conclusion:
Our results suggest that patients with acute HF complicating acute MI may benefit from being on statin therapy. Prospective clinical trials are required to validate these findings.
Deel deze pagina met collega's en vrienden: