
SHIFT: Vermindering van 1e, 2e en 3e HF heropnames met ivabradine
Literatuur - Borer JS et al, Eur Heart J 2012; DOI: 10.1093/eurheartj/ehs259. - Eur Heart J 2012; DOI: 10.1093/eurheartj/ehs259.
Post hoc analysis of data from the SHIFT trial studied effect of adding ivabradine to standard heart failure therapy on HF readmissions in patients with systolic heart failure
Borer JS, Böhm M, Ford I, et al.
Eur Heart J 2012; DOI: 10.1093/eurheartj/ehs259.
Achtergrond
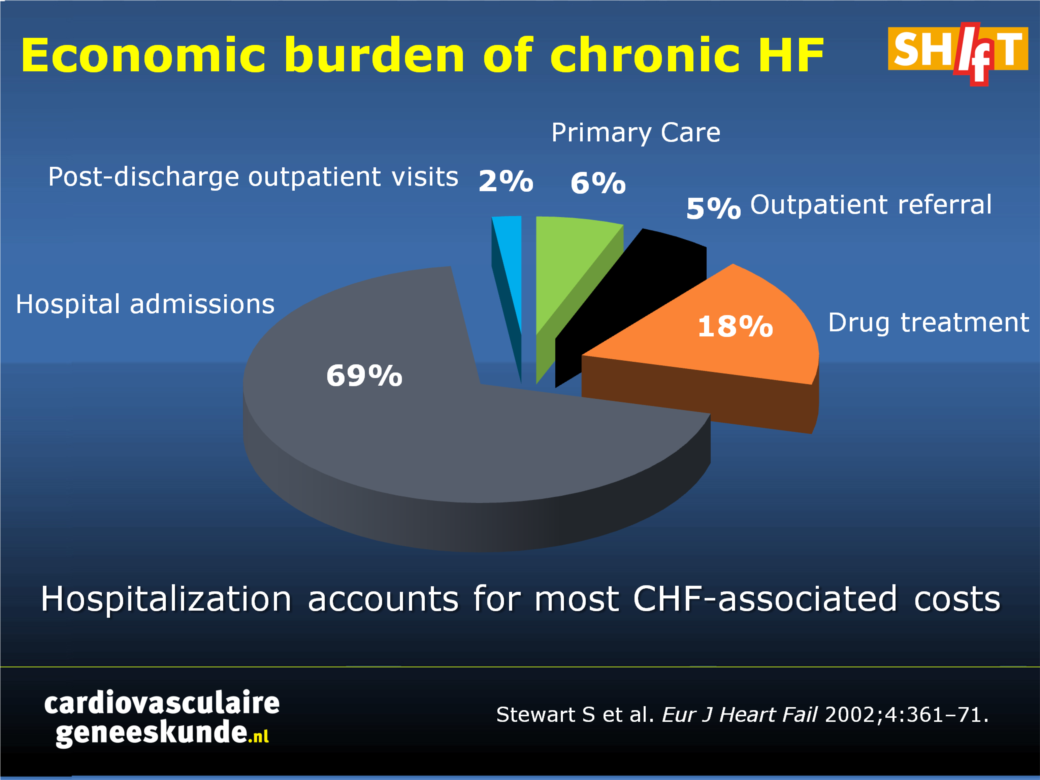
Mensen met hartfalen worden vaak opgenomen in het ziekenhuis als gevolg van verergering van hun symptomen. Eenmaal opgenomen volgt een heropname in veel gevallen [1], met een 3-maand tot 1 jaar rehospitalisatie variërend tussen de 30 en 50% [2-4]. Verslechterend HF veroorzaakt ziekenhuisopname; terugkerende ziekenhuisopname kan uiteindelijk leiden tot de dood [5-7]. De economische last van HF neemt toe [8]; HF-ziekenhuisopnamen zijn goed voor tweederde van de kosten [9] (figuur 1)
Figuur 1. Economische last van chronisch HF
Klik op afbeelding om als PPT te downloaden
De meeste evaluaties van HF therapie zijn gericht op time-to-first event analyses; behandeling na de initiële gebeurtenis wordt vaak niet in aanmerking genomen.
In deze post-hoc analyse van de SHIFT (Systolic Heart failure treatment with the If inhibitor ivabradine Trial) [10], werd het effect bekeken van een voortgezette behandeling met ivabradine op terugkerende ziekenhuisopnames voor verslechtering HF.
Belangrijkste resultaten
- Ivabradinebehandeling werd in verband gebracht met minder totale ziekenhuisopnames (902 versus 1211 met placebo; incidence rate ratio 0,75, 95% CI 0,65 tot 0,87, p = 0,0002)
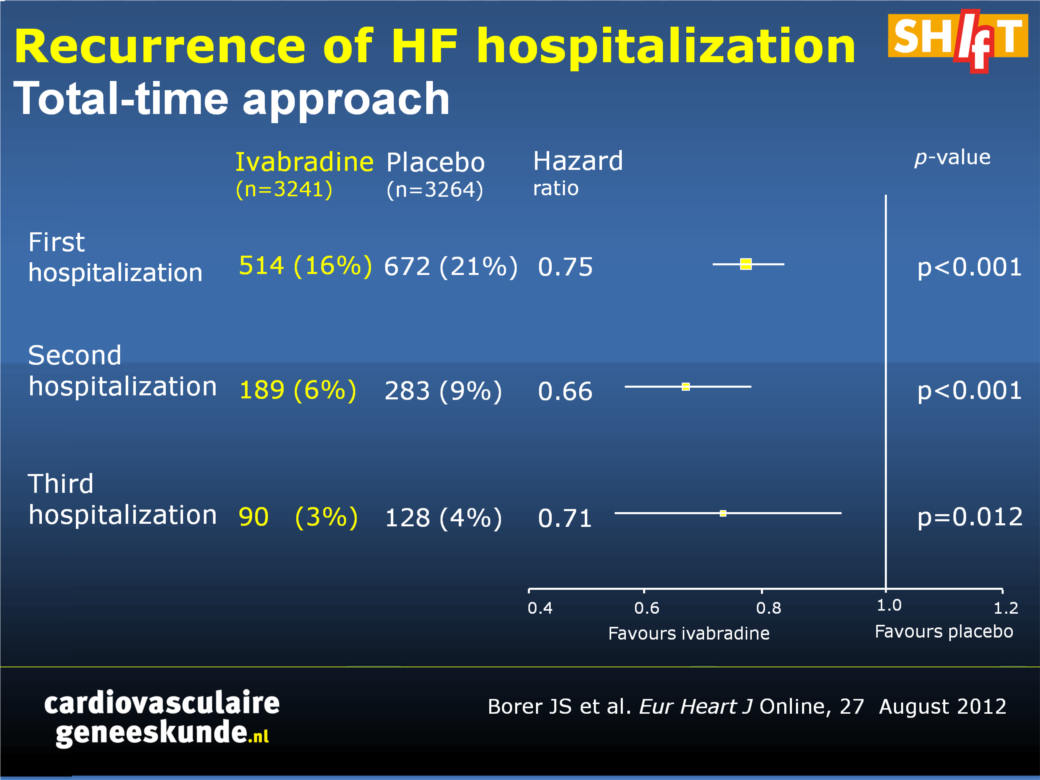
- Gedurende bijna 2 jaar follow-up hadden ivabradine patiënten een lager optreden van zowel de tweede ziekenhuisopname (HR 0,66, 95% CI 0,55 tot 0,79, p <0,001) als de derde ziekenhuisopname (HR 0,71, 95% CI 0,54 tot 0,93, P = 0,0012 ) voor het verergeren van hartfalen (figuur 2).
Figuur 2. Herhaling van HF ziekenhuisopname (totale-time benadering)
Klik op afbeelding om als PPT te downloaden
Conclusie
Ivabradine toegevoegd aan standaard hartfalen therapie verminderde HF heropnames met een derde bij patiënten met systolisch hartfalen in vergelijking met patiënten die de standaard behandeling kregen. Dit voordeel zal waarschijnlijk de kwaliteit van leven van patiënten verbeteren en zorgkosten aanzienlijk verminderen.
Redactioneel commentaar [11]
Dit spreekt voor ivabradine door te focussen op het geclaimde effect van het middel dat het in staat is om een tweede of derde ziekenhuisopnames te voorkomen, in plaats van simpelweg te richten op een eerste event in de studie.Deze benadering kan nuttig zijn omdat 472 patiënten twee of meer hospitalisaties voor hartfalen hadden en er 20.113 hospitalisaties voor hartfalen waren en 940 cardiovasculaire sterfgevallen in totaal, dat wil zeggen, 44% van alle hartfalen ziekenhuisopnames en 42% van de cardiovasculaire sterfgevallen waren 'genegeerd 'in de' time to first event' analyse.
Referenties
1. Dunlay SM, Redfield MM, Weston SA, et al. Hospitalizations after heart failure diagnosis a community perspective. J Am Coll Cardiol 2009;54:1695–1702.2. Haldeman GA, Croft JB, Giles WH, Rashidee A. Hospitalization of patients with heart failure: National Hospital Discharge Survey, 1985 to 1995. Am Heart J 1999;137:352–360.
3. Tsuchihashi M, Tsutsui H, Kodama K, et al. Medical and socioenvironmental predictors of hospital readmission in patients with congestive heart failure. Am Heart J 2001;142:E7.
4. Vinson JM, Rich MW, Sperry JC, et al. Early readmission of elderly patients with congestive heart failure. J Am Geriatr Soc 1990;38:1290–1295
5. Setoguchi S, Stevenson LW, Schneeweiss S. Repeated hospitalizations predict mortality in the community population with heart failure. Am Heart J 2007;154:260–266.
6. Abrahamsson P, Dobson J, Granger CB, et al. Impact of hospitalization for acute coronary events on subsequent mortality in patients with chronic heart failure. Eur Heart J 2009;30:338–345.
7. Solomon SD, Dobson J, Pocock S, et al. Influence of nonfatal hospitalization for heart failure on subsequent mortality in patients with chronic heart failure. Circulation 2007;116:1482–1487.
8. Liao L, Allen LA, Whellan DJ. Economic burden of heart failure in the elderly. Pharmacoeconomics 2008;26:447–462.
9. Stewart S, Jenkins A, Buchan S, et al. The current cost of heart failure to the National Health Service in the UK. Eur J Heart Fail 2002;4:361–371.
10. Swedberg K, Komajda M, Böhm M, et al. Ivabradine and outcomes in chronic heart failure (SHIFT): a randomized placebo-controlled trial. Lancet 2010;376:875–885.
11. Anker SD, McMurray JJV. Time to move on from 'time-to-first': should all events be included in the analysis of clinical trials? Eur Heart J 2012; DOI: 10.1093/eurheartj/ehs277.
Abstract
AimsWe explored the effect of treatment with ivabradine, a pure heart rate-slowing agent, on recurrent hospitalizations for worsening heart failure (HF) in the SHIFT trial.
Methods and results
SHIFT was a double-blind clinical trial in which 6505 patients with moderate-to-severe HF and left ventricular systolic dysfunction, all of whom had been hospitalized for HF during the preceding year, were randomized to ivabradine or to placebo on a background of guideline-recommended HF therapy (including maximized β-blockade). In total, 1186 patients experienced at least one additional HF hospitalization during the study, 472 suffered at least two, and 218 suffered at least 3. Patients with additional HF hospitalizations had more severe disease than those without. Ivabradine was associated with fewer total HF hospitalizations [902 vs. 1211 events with placebo; incidence rate ratio, 0.75, 95% confidence interval (CI), 0.65-0.87, P = 0.0002] during the 22.9-month median follow-up. Ivabradine-treated patients evidenced lower risk for a second or third additional HF hospitalization [hazard ratio (HR): 0.66, 95% CI, 0.55-0.79, P < 0.001 and HR: 0.71, 95% CI, 0.54-0.93, P = 0.012, respectively]. Similar observations were made for all-cause and cardiovascular hospitalizations.
Conclusion
Treatment with ivabradine, on a background of guidelines-based HF therapy, is associated with a substantial reduction in the likelihood of recurrent hospitalizations for worsening HF. This benefit can be expected to improve the quality of life and to substantially reduce health-care costs.
Deel deze pagina met collega's en vrienden: