
Vorapaxar in post-MI patiënten
Literatuur - Scirica BM et al, Lancet. 2012 Aug 24 - Lancet. 2012 Aug 24
Vorapaxar for secondary prevention of thrombotic events for patients with previous myocardial infarction: a prespecified subgroup analysis of the TRA 2°P-TIMI 50 trial
Scirica BM, Bonaca MP, Braunwald E, et al; for the TRA 2°P-TIMI 50 Steering Committee Investigators.
Lancet. 2012 Aug 24. [Epub]
Achtergrond
Patiënten met een voorgeschiedenis van myocardinfarct hebben een aanzienlijk risico van terugkerende trombotische events, ondanks secundaire preventie [1]. De werkzaamheid en veiligheid van vorapaxar, een krachtige en selectieve antagonist van de protease-activated receptor 1, zijn bestudeerd in de Thrombin Receptor Antagonist in Secondary Prevention of Atherothrombotic Ischemic Events (TRA 2P-TIMI 50) studie [2]. In de totale studie, waarin 26.449 patiënten met een voorgeschiedenis van MI, ischemische beroerte of perifeer arterieel vaatlijden gerandomiseerd werden naar vorapaxar of placebo bovenop standaard therapie, werd het optreden van cardiovasculaire sterfte, MI of beroerte aanzienlijk verminderd door vorapaxar, maar het optreden van intracraniële bloeding verdubbelde.Omdat langdurige plaatjesremmende therapie verschillende voordelen kan hebben bij patiënten met een hartinfarct [3] in vergelijking met patiënten met een beroerte en perifere arteriële ziekte [4-6], werd de subgroep van 17.779 patiënten met een voorgeschiedenis van MI geanalyseerd in deze studie.
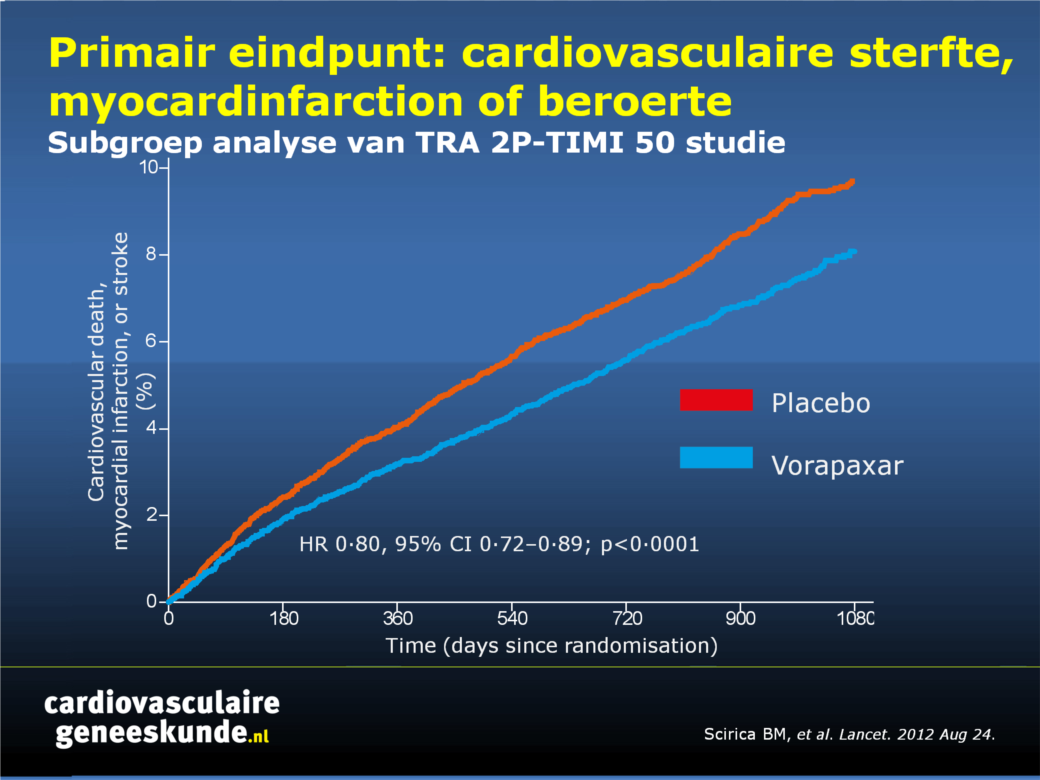
Belangrijkste resultaten
Na 2,5 jaar follow-up was het optreden van cardiovasculaire sterfte, MI of beroerte aanzienlijk verminderd in de vorapaxar-groep vergeleken met de placebogroep, hoewel vorapaxar ook geassocieerd was met een verhoogd risico op bloedingen, maar niet intracraniële bloedingen:- Primair eindpunt: 8,1% versus 9,7%, HR 0,80, CI 0,72-0.89, p <0,0001
- Matige of ernstige bloedingen: 3,4% versus 2,1%, HR 1,61, CI 1,31-1.97, p <0,0001
- intracraniële bloeding: 0,6% versus 0,4%, p = 0,076
Conclusie
Vorapaxar verminderde het risico op cardiovasculaire dood of ischemische gebeurtenissen. Omdat vorapaxar het risico van gevaarlijke bloedingen verhoogde, zullen clinici zorgvuldig moeten beoordelen welke groepen patiënten zullen profiteren van de behandeling. Vorapaxar zou nuttig kunnen zijn in een populatie met een voorgeschiedenis van MI, maar zonder voorgeschiedenis van een beroerte of TIA, leeftijd onder de 75, en een gewicht meer dan 60 kg, waarbij de cardiovasculaire voordelen van een langdurige behandeling waarschijnlijk opwegen tegen de negatieve gezondheidsrisico’s voor de patiënt in verband met een hogere kans op bloedingen.
Redactioneel commentaar [7]
"De resultaten van deze studie geven verdere ondersteuning aan het toevoegen van meer potente langdurige anti trombotische therapie voor patiënten die eerder een hartaanval hadden. Echter, de uitdaging is - net als bij alle strategieën van dit type - de voordelen tegen het verhoogde risico op bloedingen af te wegen."
Referenties
- Steg PG, Bhatt DL, Wilson PW, et al. One-year cardiovascular event rates in outpatients with atherothrombosis. JAMA 2007;297: 1197–206.
- Morrow DA, Braunwald E, Bonaca MP, et al. Vorapaxar in the secondary prevention of atherothrombotic events. N Engl J Med 2012;366:1404–13.
- Bhatt DL, Flather MD, Hacke W, et al. Patients with prior myocardial infarction, stroke, or symptomatic peripheral arterial disease in the CHARISMA trial. J Am Coll Cardiol 2007; 49: 1982–88.
- Diener HC, Bogousslavsky J, Brass LM, et al. Aspirin and clopidogrel compared with clopidogrel alone after recent ischaemic stroke or transient ischaemic attack in high-risk patients (MATCH): randomised, double-blind, placebo-controlled trial. Lancet 2004;364: 331–37.
- Fowkes FG, Price JF, Stewart MC, et al. Aspirin for prevention of cardiovascular events in a general population screened for a low ankle brachial index: a randomized controlled trial. JAMA 2010;303: 841–48.
- Sacco RL, Diener HC, Yusuf S, et al. Aspirin and extended-release dipyridamole versus clopidogrel for recurrent stroke. N Engl J Med 2008;359:1238–51
- James S, Held C. Improving long-term outcome after myocardial infarction. Lancet. 2012 Aug 24. [Epub ahead of print]
Abstract
Background:Vorapaxar inhibits platelet activation by antagonising thrombin-mediated activation of the protease-activated receptor 1 on human platelets. The effect of adding other antiplatelet drugs to aspirin for long-term secondary prevention of thrombotic events in stable patients with previous myocardial infarction is uncertain. We tested this effect in a subgroup of patients from the Thrombin Receptor Antagonist in Secondary Prevention of Atherothrombotic Ischemic Events (TRA 2°P)-TIMI 50 trial.
Methods:
In TRA 2°P-TIMI 50-a randomised, placebo-controlled, parallel trial-we randomly assigned patients with a history of atherothrombosis to receive vorapaxar (2•5 mg daily) or matching placebo in a 1:1 ratio. Patients, and those giving treatment, assessing outcomes, and analysing results were masked to treatment allocation. Patients with a qualifying myocardial infarction within the previous 2 weeks to 12 months were analysed as a pre-defined subgroup. The primary efficacy endpoint was cardiovascular death, myocardial infarction, or stroke, analysed by intention to treat. We analysed events by Kaplan-Meier analysis and compared groups with a Cox proportional hazard model. TRA 2°P-TIMI 50 is registered at ClinicalTrials.gov (NCT00526474).
Findings:
17 779 of 26 449 patients had a qualifying myocardial infarction and were assigned treatment (8898 to vorapaxar and 8881 to placebo). Median follow-up was 2•5 years (IQR 2•0-2•9). Cardiovascular death, myocardial infarction, or stroke occurred in 610 of 8898 patients in the vorapaxar group and 750 of 8881 in the placebo group (3-year Kaplan-Meier estimates 8•1%vs 9•7%, HR 0•80, 95% CI 0•72-0•89; p<0•0001). Moderate or severe bleeding was more common in the vorapaxar group versus the placebo group (241/8880 [3•4%, 3-year Kaplan-Meier estimate] vs 151/8849 [2•1%, 3-year Kaplan-Meier estimate], HR 1•61, 95% CI 1•31-1•97; p<0•0001). Intracranial haemorrhage occurred in 43 of 8880 patients (0•6%, 3-year Kaplan-Meier estimate) with vorapaxar versus 28 of 8849 (0•4%, 3-year Kaplan-Meier estimate) with placebo (p=0•076). Other serious adverse events were equally distributed between groups.
Interpretation:
For patients with a history of myocardial infarction, inhibition of protease-activated receptor 1 with vorapaxar reduces the risk of cardiovascular death or ischaemic events when added to standard antiplatelet treatment, including aspirin, and increases the risk of moderate or severe bleeding.
Deel deze pagina met collega's en vrienden: