
BMI beïnvloedt frequentie CV aandoeningen bij hypertensie
Literatuur - Weber MA, Jamerson K, Bakris GL, et al. - Lancet. 2013 Feb 16;381(9866):537-45. doi: 10.1016/S0140-6736(12)61343-9.
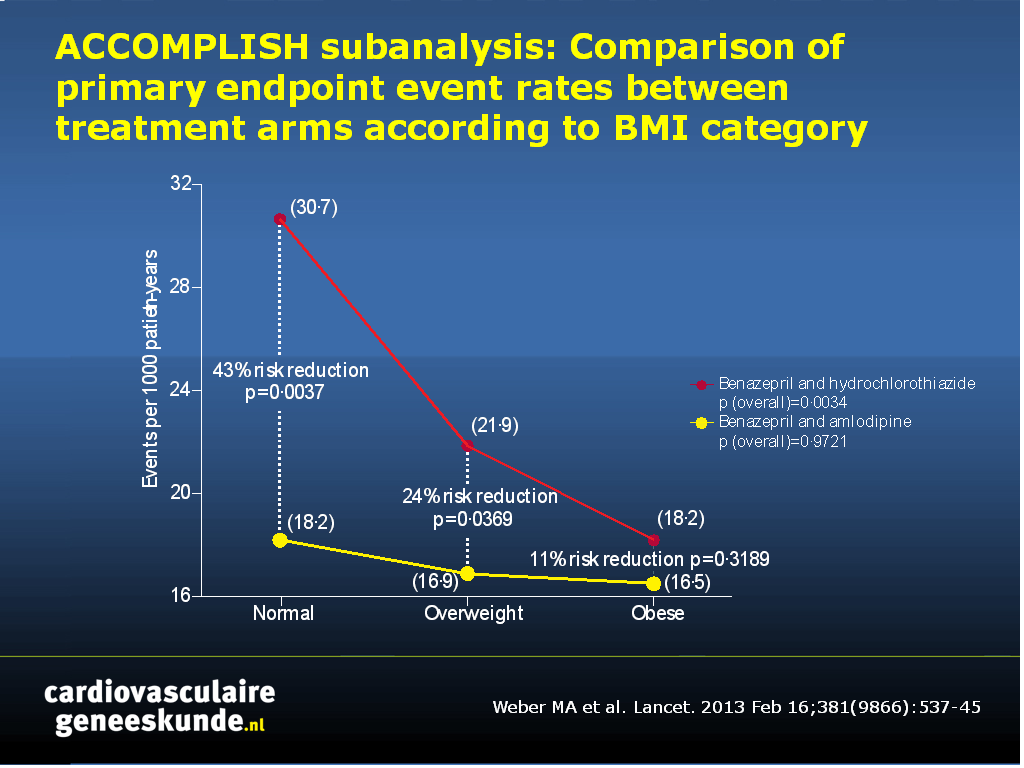
Effects of body size and hypertension treatments on cardiovascular event rates: subanalysis of the ACCOMPLISH randomised controlled trial.
Weber MA, Jamerson K, Bakris GL, et al.Lancet. 2013 Feb 16;381(9866):537-45. doi: 10.1016/S0140-6736(12)61343-9.
Achtergrond
Het wordt algemeen erkend dat obesitas geassocieerd is met een hoge incidentie cardiovasculaire (CV) aandoeningen. Het is opvallend dat individuen met een normaal lichaamsgewicht met bevestigde hart- en vaatziekten (HVZ) vaker aan CV aandoeningen lijken te lijden [1-3]. Ook slanke hypertensieve mensen hebben een hogere incidentie van nadelige CV uitkomst dan obese mensen [4-6]. Een klinische trial van antihypertensie behandeling liet een hogere CV frequentie zien in slanke mensen, in tegenstelling tot obese individuen [7]. Helaas kon uit deze studie niet geconcludeerd worden of deze ‘obesitas paradox’ het gevolg was van aangeboren klinische eigenschappen, of een effect van medicijnen, aangezien alle patiënten actief werden behandeld.De gerandomiseerde, dubbelblinde, multicenter Avoiding Cardiovascular Events through Combination Therapy in Patients Living with Systolic Hypertension (ACCOMPLISH) trial biedt een mogelijkheid om de effecten van lichaamsgewicht en verschillende behandelstrategieën te bestuderen in hoog-risico hypertensieve patiënten, aangezien deze studie CV uitkomsten vergelijkt in groepen behandeld met diuretica (benazepril + hydrochlorothiazide) vs niet-diuretica (benazepril + amlodipine).
Belangrijkste resultaten
- De frequentie van CV uitkomsten is significant lager in obese (BMI>30) hypertensieve patiënten, in vergelijking tot mensen met normaal lichaamsgewicht (BMI: 20-25) (HR: 0.74, 95%CI: 0.59-0.92, P=0.0066)
- Verschillende behandelstrategieën waren even effectief in het verminderen van CV eindpunt frequentie in obese patiënten. De eindpunt frequentie was lager in patiënten met overgewicht (BMI: 25-30) die behandeld werden met benazepril en amlodipine. Dit verschil was groter in patiënten met een normaal lichaamsgewicht.
Conclusies
Het soort behandeling is een determinant van de relatie tussen lichaamsgewicht en CV uitkomsten. Beide behandelingsstrategieën waren effectief in obese patiënten. Slanke patiënten zijn echter beter beschermd tegen CV aandoeningen als ze een behandeling krijgen die een calciumkanaalblokker bevat, in plaats van thiazide-gebaseerde therapie. De auteurs bespreken dat hypertensie in obese en slanke mensen waarschijnlijk het gevolg is van een andere onderliggende pathofysiologie, hetgeen het verschil in effect van behandeling in verschillende gewichtscategorieën mogelijk kan verklaren.Download CVG accomplish 2013.pptx
Referenties
1.Curtis JP, Selter JG, Wang Y, et al. The obesity paradox: body mass index and outcomes in patients with heart failure. Arch Intern Med 2005; 165: 55–61.2. Gruberg L, Weissman NJ, Waksman R, et al. The impact of obesity on the short-term and long-term outcomes after percutaneous coronary intervention: the obesity paradox? J Am Coll Cardiol 2002; 39: 578–84.
3. Kang X, Shaw LJ, Hayes SW, et al. Impact of body mass index on cardiac mortality in patients with known or suspected coronary artery disease undergoing myocardial perfusion single-photon emission computed tomography. J Am Coll Cardiol 2006; 47: 1418–26.
4. Barrett-Connor E, Khaw K. Is hypertension more benign when associated with obesity? Circulation 1985; 72: 53–60.
5. Goldbourt U, Holtzman E, Cohen-Mandelzweig L, Neufeld HN. Enhanced risk of coronary heart disease mortality in lean hypertensive men. Hypertension 1987; 10: 22–28.
6.Carman WJ, Barrett-Connor E, Sowers M, Khaw K. Hypertension/risk factors: higher risk of cardiovascular mortality among lean hypertensive individuals in Tecumesh, Michigan. Circulation 1994; 89: 703–11.
7.Uretsky S, Messerli FH, Bangalore S, et al. Obesity paradox in patients with hypertension and coronary artery disease. Am J Med 2007; 120: 863–70.
8.Jamerson K, Weber MA, Bakris GL, et al. Benazepril plus amlodipine or hydrochlorothiazide for hypertension in high-riskpatients. N Engl J Med 2008; 359: 2417–28.
Abstract
BACKGROUND:
In previous clinical trials in high-risk hypertensive patients, paradoxically higher cardiovascular event rates have been reported in patients of normal weight compared with obese individuals. As a prespecified analysis of the Avoiding Cardiovascular Events through Combination Therapy in Patients Living with Systolic Hypertension (ACCOMPLISH) trial, we aimed to investigate whether the type of hypertension treatment affects patients' cardiovascular outcomes according to their body size.
METHODS:
On the basis of body-mass index (BMI), we divided the full ACCOMPLISH cohort into obese (BMI ≥30, n=5709), overweight (≥25 to <30, n=4157), or normal weight (<25, n=1616) categories. The ACCOMPLISH cohort had already been randomised to treatment with single-pill combinations of either benazepril and hydrochlorothiazide or benazepril and amlodipine. We compared event rates (adjusted for age, sex, diabetes, previous cardiovascular events, stroke, or chronic kidney disease) for the primary endpoint of cardiovascular death or non-fatal myocardial infarction or stroke. The analysis was by intention to treat. This trial is registered with ClinicalTrials.gov, number NCT00170950.
FINDINGS:
In patients allocated benazepril and hydrochlorothiazide, the primary endpoint (per 1000 patient-years) was 30•7 in normal weight, 21•9 in overweight, and 18•2 in obese patients (overall p=0•0034). However, in those allocated benazepril and amlodipine, the primary endpoint did not differ between the three BMI groups (18•2, 16•9, and 16•5, respectively; overall p=0•9721). In obese individuals, primary event rates were similar with both benazepril and hydrochlorothiazide and benazepril and amlodipine, but rates were significantly lower with benazepril and amlodipine in overweight patients (hazard ratio 0•76, 95% CI 0•59-0•94; p=0•0369) and those of normal weight (0•57, 0•39-0•84; p=0•0037).
INTERPRETATION:
Hypertension in normal weight and obese patients might be mediated by different mechanisms. Thiazide-based treatment gives less cardiovascular protection in normal weight than obese patients, but amlodipine-based therapy is equally effective across BMI subgroups and thus offers superior cardiovascular protection in non-obese hypertension.
Deel deze pagina met collega's en vrienden: