
AMPLIFY-EXT: apixaban bij preventie van DVT en longembolie
Literatuur - Agnelli G, Buller HR, Cohen A, et al - N Engl J Med 2013;368:699-708Apixaban for Extended Treatment of Venous Thromboembolism
Giancarlo Agnelli, M.D., Harry R. Buller, M.D., Ph.D., Alexander Cohen, M.D., Madelyn Curto, D.V.M., Alexander S. Gallus, M.D., Margot Johnson, M.D., Anthony Porcari, Ph.D., Pharm.D., Gary E. Raskob, Ph.D., and Jeffrey I. Weitz, M.D. for the AMPLIFY-EXT Investigators
N Engl J Med 2013; 368:699-708February 21, 2013DOI: 10.1056/NEJMoa1207541
Achtergrond
Veneuze trombo-embolie is de derde oorzaak van cardiovasculaire sterfte [1]. Antistolling is de hoeksteen van de behandeling; richtlijnen bevelen een behandeling aan gedurende 3 maanden of langer [2,3]. Hoewel warfarine effectief is voor de preventie van recidiverende veneuze trombo-embolie, maakt het bloedingsrisico, samen met de noodzaak van regelmatige laboratoriumcontrole en dosisaanpassingen, lange-termijnbehandeling lastig.Apixaban is een orale factor Xa remmer die wordt toegediend in vaste doseringen waarbij regelmatige controle en dosisaanpassingen niet nodig zijn. Bij een dosering van 5 mg tweemaal daags is apixaban effectief voor de preventie van stroke in patiënten met atriumfibrilleren. Bij een dosering van 2,5 mg tweemaal daags is het effectief voor tromboprofylaxe na grote orthopedische operaties [5-7].
In de AMPLIFY-EXT studie werden 2.486 VTE patiënten gerandomiseerd naar placebo of apixaban (2,5 of 5 mg tweemaal daags) voor nog eens 12 maanden na voltooiing van een eerste standaard antistolling behandeling gedurende 6-12 maanden. Het primaire effectiviteits-eindpunt was het gecombineerde eindpunt van symptomatische, herhaalde VTE (niet-fataal DVT of niet-fataal PE) en sterfte door alle oorzaken. Sterfte werd geclassificeerd als VTE-gerelateerd, cardiovasculair gerelateerd, als gevolg van bloedingen of door andere oorzaken.
Belangrijkste resultaten:
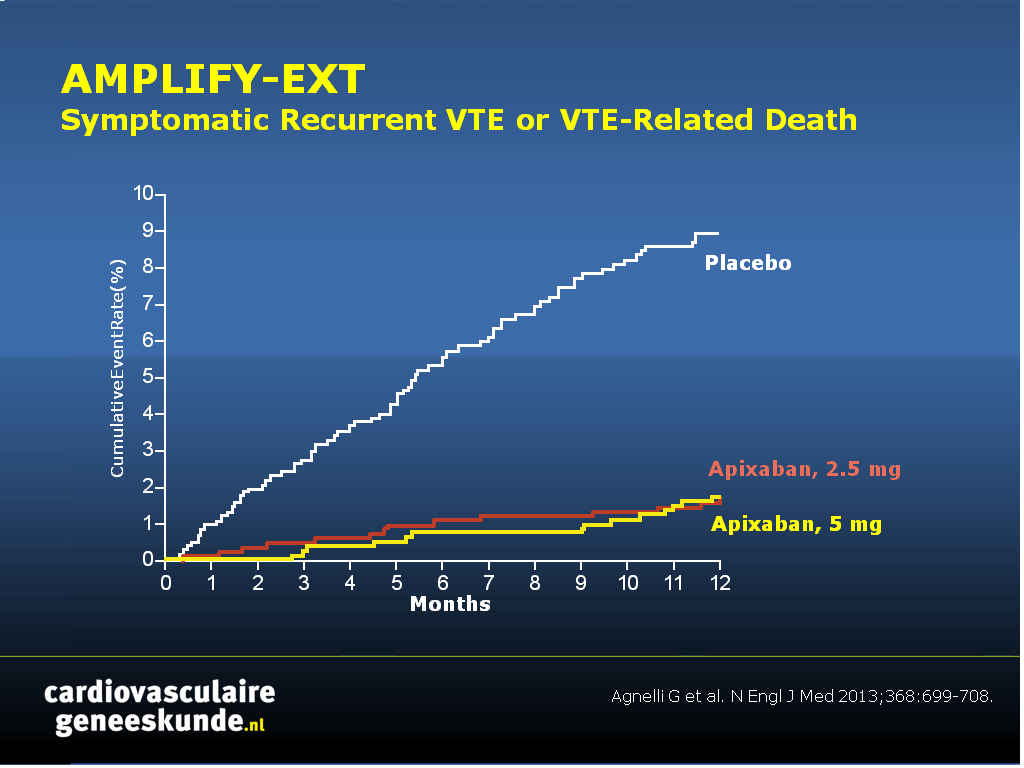
Bij beide doseringen was behandeling met apixaban geassocieerd met een grote reductie in klinische events zonder een toename van ernstige bloedingen.Recidiverende VTE of VTE-gerelateerde sterfte(fig. 1)
- 1,7% voor lage dosis apixaban versus 1,7% voor een hoge dosis apixaban versus 8,8% voor placebo, RR 0,19 (0,11 - 0,33) voor een lage dosis apixaban en 0,20 (0,11-0,34) voor een hoge dosis apixaban
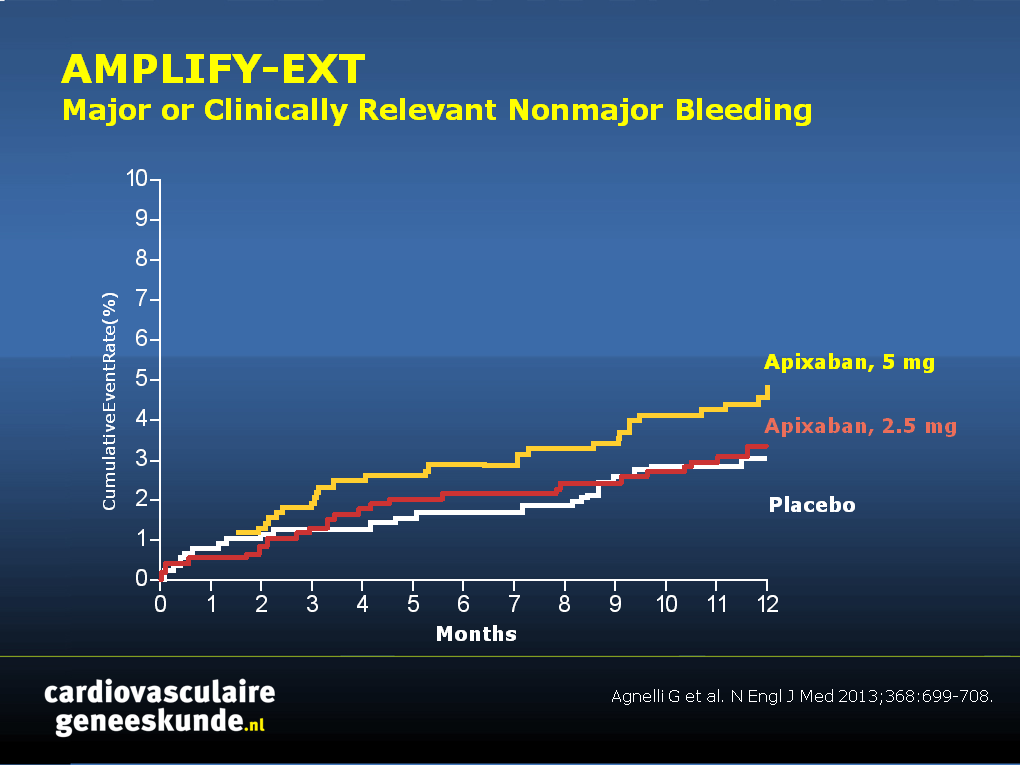
Ernstige of klinisch relevante bloedingen (fig. 2)
- 3,2% voor lage dosis apixaban versus 4,3% voor een hoge dosis apixaban versus 2,7% voor placebo, RR 1. 20 (0.69 - 2.10) voor een lage dosis placebo en 1,62 (0.96 - 2,73) voor een hoge dosis apixaban
Conclusie:
Zowel de 2,5-mg dosis als de 5 mg dosis apixaban verminderde het risico op recidiverende veneuze trombo-embolie (fataal of niet-fataal) waarbij het optreden van ernstige bloedingen laag was en vergelijkbaar met die van de placebo groep.Redactioneel commentaar [7]:
“Voor patiënten met een hoger risico op recidiverende VTE zijn de nieuwe orale anticoagulantia aantrekkelijke alternatieven voor warfarine; hoewel het bloedingsrisico in ogenschouw moet worden genomen. De bevinding dat een lage profylactische dosis apixaban dezelfde werkzaamheid als de volledige therapeutische dosis heeft, zonder verhoogd risico op ernstige bloedingen, kan de risico-baten verhouding doen omslaan ten gunste van langdurige behandeling voor deze patiëntenpopulatie. Het brede therapeutisch venster van dit middel maakt gebruik van een lagere dosis mogelijk met behoud van een hoge effectiviteit met geen of slechts een minimale verhoging van bloedingen.”Download CVG AMPLIFY EXT 2013.pptx
Referenties:
1. Goldhaber SZ, Bounameaux H. Pulmonary embolism and deep vein thrombosis. Lancet 2012;379:1835-46.2. Torbicki A, Perrier A, Konstantinides S, et al. Guidelines on the diagnosis and management of acute pulmonary embolism: the Task Force for the Diagnosis and Management of Acute Pulmonary Embolism of the European Society of Cardiology (ESC). Eur Heart J 2008;29:2276-315.
3. Kearon C, Akl EA, Comerota AJ, et al. Antithrombotic therapy for VTE disease: Antithrombotic Therapy and Prevention of Thrombosis. 9th ed.: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest 2012;141:Suppl:e419S-e494S.
4. Granger CB, Alexander JH, McMurray JJ, et al. Apixaban versus warfarin in patients with atrial fibrillation. N Engl J Med 2011;365:981-92.
5. Connolly SJ, Eikelboom J, Joyner C, et al. Apixaban in patients with atrial fibrillation. N Engl J Med 2011;364:806-17.
6. Raskob GE, Gallus AS, Pineo GF, et al. Apixaban versus enoxaparin for thromboprophylaxis after hip or knee replacement: pooled analysis of major venous thromboembolism and bleeding in 8464 patients from the ADVANCE-2 and ADVANCE-3 trials. J Bone Joint Surg Br 2012;94:257-64.
7. Connors JM. Extended Treatment of Venous Thromboembolism N Engl J Med 2013; 368:767-769
Abstract
Background:Apixaban, an oral factor Xa inhibitor that can be administered in a simple, fixed-dose regimen, may be an option for the extended treatment of venous thromboembolism.
Methods:
In this randomized, double-blind study, we compared two doses of apixaban (2.5 mg and 5 mg, twice daily) with placebo in patients with venous thromboembolism who had completed 6 to 12 months of anticoagulation therapy and for whom there was clinical equipoise regarding the continuation or cessation of anticoagulation therapy. The study drugs were administered for 12 months.
Results:
A total of 2486 patients underwent randomization, of whom 2482 were included in the intention-to-treat analyses. Symptomatic recurrent venous thromboembolism or death from venous thromboembolism occurred in 73 of the 829 patients (8.8%) who were receiving placebo, as compared with 14 of the 840 patients (1.7%) who were receiving 2.5 mg of apixaban (a difference of 7.2 percentage points; 95% confidence interval [CI], 5.0 to 9.3) and 14 of the 813 patients (1.7%) who were receiving 5 mg of apixaban (a difference of 7.0 percentage points; 95% CI, 4.9 to 9.1) (P<0.001 for both comparisons). The rates of major bleeding were 0.5% in the placebo group, 0.2% in the 2.5-mg apixaban group, and 0.1% in the 5-mg apixaban group. The rates of clinically relevant nonmajor bleeding were 2.3% in the placebo group, 3.0% in the 2.5-mg apixaban group, and 4.2% in the 5-mg apixaban group. The rate of death from any cause was 1.7% in the placebo group, as compared with 0.8% in the 2.5-mg apixaban group and 0.5% in the 5-mg apixaban group.
Conclusions:
Extended anticoagulation with apixaban at either a treatment dose (5 mg) or a thromboprophylactic dose (2.5 mg) reduced the risk of recurrent venous thromboembolism without increasing the rate of major bleeding.
Deel deze pagina met collega's en vrienden: