
Effect statine en lichaamsbeweging op mortaliteit
Literatuur - Kokkinos PF, Faselis C, Myers J, et al. Lancet 2012; - Lancet 2012; DOI:10.1016/S0140-6736(12)61426-3.
Interactive effects of fitness and statin treatment on mortality risk in veterans with dyslipidemia: a cohort study.
Kokkinos PF, Faselis C, Myers J, et al.
Lancet 2012; DOI:10.1016/S0140-6736(12)61426-3.
Achtergrond
Behandeling met statines vermindert morbiditeit en mortaliteit aanzienlijk bij patiënten met coronaire hartziekte [1-3]. Ook mensen met een risico op hart- en vaatziekten kunnen baat hebben bij behandeling met een statine [4-7].Veranderingen in levensstijl zijn ook belangrijk om het cardiovasculaire risico te verminderen [8,9]. Er zijn weinig gegevens beschikbaar over de gecombineerde effecten van fitness en statinebehandeling. Deze studie onderzocht zowel de afzonderlijke als de gecombineerde effecten van statinebehandeling en inspanningscapaciteit op het risico op sterfte door alle oorzaken in dyslipidemische veteranen. Gegevens van 10.043 mensen met dyslipidemie behandeld in 2 Veterans Affairs Medical Centers werden geanalyseerd; deelnemers werden gevolgd gedurende een mediane periode van 10 jaar, gedurende welke tijd bijna een kwart van hen stierf.
Belangrijkste resultaten
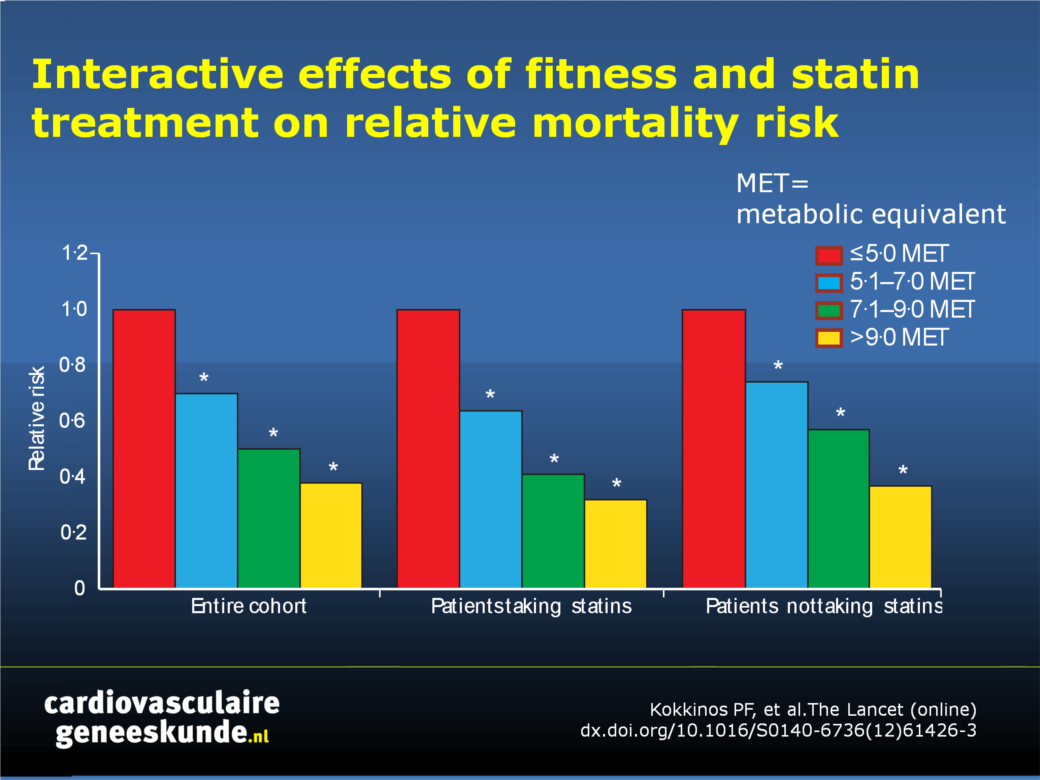
- Patiënten die statines kregen en fysiek fit waren hadden tot 70% vermindering van het risico van overlijden tijdens de follow-up periode, vergeleken met de minst fysiek fitte patiënten die statines kregen (P <0,0001).
- Fysieke fitheid had ook een onafhankelijk effect op het mortaliteitsrisico bij patiënten die geen statines gebruikten, waardoor de kans op overlijden tijdens de follow-up met maar liefst 47% afnam (p <0,0001).
Conclusie
De combinatie van statinebehandeling en een voldoende hoge inspanningscapaciteit verlaagt de kans op overlijden aanzienlijk en meer dan een van beide alleen. Deze bevinding suggereert dat een betere conditie een aantrekkelijke aanvulling is op behandeling met statines of een alternatief wanneer statines niet kunnen worden gebruikt.
Redactioneel commentaar [10]
"De onderwaardering van fysieke activiteit in de klinische praktijk is onacceptabel. Het voorschrijven van fysieke activiteit moet op een lijn worden gelegd met het voorschrijven van geneesmiddelen. De kosten om fysiek actief te worden zijn lager dan die van het kopen van geneesmiddelen, en matig intensieve lichaamsbeweging heeft minder bijwerkingen. In tegenstelling tot statines, zou fysieke activiteit deel moeten uitmaken van het dagelijks leven. "Download als PowerPoint
Klik op afbeelding
Figuur 1:
Relatieve sterfterisico per fitheidscategorie* Significant verschillend van referentiegroep. MET = metabool equivalent.
Referenties
1. West of Scotland Coronary Prevention Study Group. Influence of pravastatin and plasma lipids on clinical events in the West of Scotland Coronary Prevention Study (WOSCOPS). Circulation 1998; 97: 1440–45.2. Pedersen TR, Olsson AG, Faergeman O, et al. Lipoprotein changes and reduction in the incidence of major coronary heart disease events in the Scandinavian Simvastatin Survival Study (4S). Circulation 1998;97: 1453–60.
3. Sacks FM, Moye LA, Davis BR, et al. Relationship between plasma LDL concentrations during treatment with pravastatin and recurrent coronary events in the Cholesterol and Recurrent Events trial. Circulation 1998; 97: 1446–52.
4. Cholesterol Treatment Trialists’ (CTT) Collaborators. Efficacy and safety of cholesterol-lowering treatment: prospective meta-analysis of data from 90 056 participants in 14 randomised trials of statins. Lancet 2005; 366: 1267–78.
5. Ray KK, Seshasai SR, Erqou S, et al. Statins and all-cause mortality in high-risk primary prevention: a meta-analysis of 11 randomized controlled trials involving 65,229 participants. Arch Intern Med 2010;170: 1024–31.
6. Taylor F, Ward K, Moore TH, et al. Statins for the primary prevention of cardiovascular disease. Cochrane Database Syst Rev 2011; CD004816.
7. Thavendiranathan P, Bagai A, Brookhart MA, Choudhry NK. Primary prevention of cardiovascular diseases with statin therapy: a meta-analysis of randomized controlled trials. Arch Intern Med 2006;166: 2307–13.
8. Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. Executive summary of the Third Report of The National Cholesterol Education Program (NCEP) expert panel on detection, evaluation, and treatment of high blood cholesterol in adults (adult treatment panel III). JAMA 2001; 285: 2486–97.
9. Grundy SM, Cleeman JI, Merz CN, et al. Implications of recent clinical trials for the National Cholesterol Education Program Adult Treatment Panel III guidelines. Circulation 2004; 110: 227–39.
10. Hallal PC and Lee IM. Prescription of physical activity: An undervalued intervention. Lancet 2012; DOI:10.1016/S0140-6736(12)61804-2.
Abstract
Background
Statins are commonly prescribed for management of dyslipidaemia and cardiovascular disease. Increased fitness is also associated with low mortality and is recommended as an essential part of promoting health. However, little information exists about the combined effects of fitness and statin treatment on all-cause mortality. We assessed the combined effects of statin treatment and fitness on all-cause mortality risk.
Methods In this prospective cohort study, we included dyslipidaemic veterans from Veterans Affairs Medical Centers in Palo Alto, CA, and Washington DC, USA, who had had an exercise tolerance test between 1986, and 2011. We assigned participants to one of four fitness categories based on peak metabolic equivalents (MET) achieved during exercise test and eight categories based on fitness status and statin treatment. The primary endpoint was all-cause mortality adjusted for age, body-mass index, ethnic origin, sex, history of cardiovascular disease, cardiovascular drugs, and cardiovascular risk factors. We assessed mortality from Veteran’s Affairs’ records on Dec 31, 2011. We compared groups with Cox proportional hazard model.
Findings
We assessed 10 043 participants (mean age 58•8 years, SD 10•9 years). During a median follow-up of 10•0 years (IQR 6•0–14•2), 2318 patients died, with an average yearly mortality rate of 22 deaths per 1000 person-years. Mortality risk was 18•5% (935/5046) in people taking statins versus 27•7% (1386/4997) in those not taking statins (p<0•0001). In patients who took statins, mortality risk decreased as fitness increased; for highly fi t individuals (>9 MET; n=694), the hazard ratio (HR) was 0•30 (95% CI 0•21–0•41; p<0•0001) compared with least fi t (≤5 METs) patients (HR 1; n=1060). For those not treated with statins, the HR for least fi t participants (n=1024) was 1•35 (95% CI 1•17–1•54; p<0•0001) and progressively decreased to 0•53 (95% CI 0•44–0•65; p<0•0001) for those in the highest fitness category (n=1498).
Interpretation
Statin treatment and increased fitness are independently associated with low mortality among dyslipidaemic individuals. The combination of statin treatment and increased fitness resulted in substantially lower mortality risk than either alone, reinforcing the importance of physical activity for individuals with dyslipidaemia
Deel deze pagina met collega's en vrienden: