
PCSK9-remmer en statines bij hypercholesterolemie
Literatuur - Roth EM, McKenney JM, Hanotin C, et al. NEJm 2012 - N Engl J Med. 2012;367:1891-900. doi: 10.1056/NEJMoa1201832.Atorvastatin with or without an antibody to PCSK9 in primary hypercholesterolemia.
Roth EM, McKenney JM, Hanotin C, et al.N Engl J Med. 2012;367:1891-900. doi: 10.1056/NEJMoa1201832.
Achtergrond
Hoewel statines zeer effectief zijn in het verlagen LDL cholesterol, bereiken veel patiënten, met name die met zeer grote initiële LDL cholesterolwaaren en met onaanvaardbare bijwerkingen met hoge dosis statines, niet de aanbevolen streefwaarden van LDL-cholesterol [1,2]. Er blijft een aanzienlijke onbeantwoorde medische behoefte aan additionele, meer effectieve therapeutische alternatieven met aanvaardbare bijwerkingsprofielen. Eerder dit jaar werden de resultaten gepubliceerd van drie fase 1 studies die de cholesterol-verlagende effecten van hetmiddel bij gezonde vrijwilligers en bij mensen met familiaire of niet-familiaire hypercholesterolemie [3].In deze studie werden 92 patiënten met een LDL-niveau meer dan 100 mg / dl ondanks behandeling met atorvastatine 10 mg bestudeerd. Patiënten werden vervolgens gerandomiseerd naar 8 weken behandeling met 80 mg atorvastatine plus de PCSK9 remmer SAR236553, 10 mg atorvastatine plus SAR236553, of 80 mg atorvastatine alleen. SAR236553 werd toegediend als een injectie eenmaal per 2 weken.
Belangrijkste resultaten
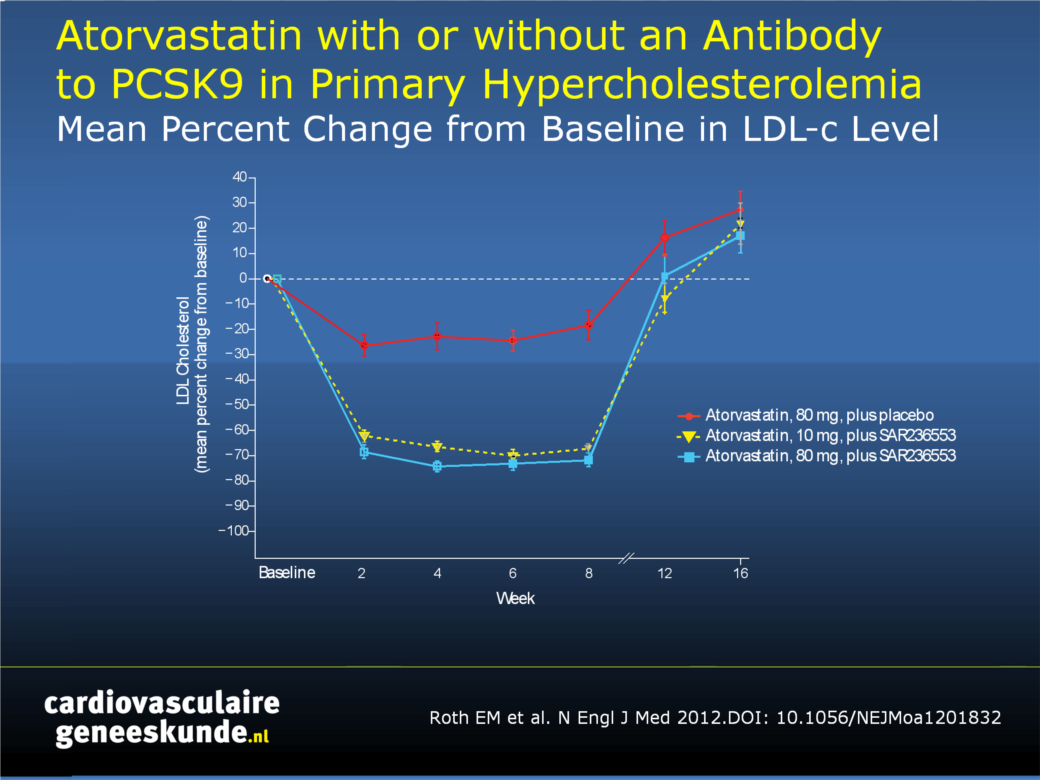
Vermindering van LDL-cholesterol ten opzichte van baseline:- SAR236553 + atorvastatine 80 mg: 73,2% ± 3,5
- SAR236553 + atorvastatine 10 mg: 66,2% ± 3,5
- atorvastatine 80 mg: 17,3% ± 3,5
100% van de patiënten in beide groepen die SAR236553 kregen bereikte LDL waarden van minder dan 100 mg / dl, vergeleken met slechts 52% van degenen die werden behandeld met atorvastatine 80 mg alleen.
Conclusie
SAR236553 komt in aanmerking voor patiënten bij wie het LDL cholesterol niet is verlaagd tot aanbevolen niveaus, hetzij vanwege een inadequate lipidenverlagende respons met hoge doseringen statines alleen of door onaanvaardbare bijwerkingen met hoge doseringen statines.
Figuur 1.
Gemiddelde procentuele verandering ten opzichte van baseline in low-density lipoprotein (LDL) cholesterol niveaus, per behandelingsgroep. (resultaten getoond voor het primaire resultaat, gemiddelde percentage verandering ten opzichte van baseline in LDL cholesterol niveaus tot week 8, berekend met gebruik van de last-observation-carried-forward (LOCF) methode)
Download als PPT
Referenties
1. Waters DD, Brotons C, Chiang CW, et al. Lipid Treatment Assessment Project 2: a multinational survey to evaluate the proportion of patients achieving low-density lipoprotein cholesterol goals. Circulation 2009;120:28-34.2. Ford ES, Li C, Pearson WS, et al. Trends in hypercholesterolemia, treatment and control among United States adults. Int J Cardiol 2010;140:226-35.
3. Stein EA, Mellis S, Yancopoulos GD, et al. Effect of a monoclonal antibody to PCSK9 on LDL cholesterol. N Engl J Med. 2012;366:1108-18.
Abstract
Background:Serum proprotein convertase subtilisin/kexin 9 (PCSK9) binds to low-density lipoprotein (LDL) receptors, increasing the degradation of LDL receptors and reducing the rate at which LDL cholesterol is removed from the circulation. REGN727/SAR236553 (designated here as SAR236553), a fully human PCSK9 monoclonal antibody, increases the recycling of LDL receptors and reduces LDL cholesterol levels.
Methods:
We performed a phase 2, multicenter, double-blind, placebo-controlled trial involving 92 patients who had LDL cholesterol levels of 100 mg per deciliter (2.6 mmol per liter) or higher after treatment with 10 mg of atorvastatin for at least 7 weeks. Patients were randomly assigned to receive 8 weeks of treatment with 80 mg of atorvastatin daily plus SAR236553 once every 2 weeks, 10 mg of atorvastatin daily plus SAR236553 once every 2 weeks, or 80 mg of atorvastatin daily plus placebo once every 2 weeks and were followed for an additional 8 weeks after treatment.
Results:
The least-squares mean (±SE) percent reduction from baseline in LDL cholesterol was 73.2±3.5 with 80 mg of atorvastatin plus SAR236553, as compared with 17.3±3.5 with 80 mg of atorvastatin plus placebo (P<0.001) and 66.2±3.5 with 10 mg of atorvastatin plus SAR236553. All the patients who received SAR236553, as compared with 52% of those who received 80 mg of atorvastatin plus placebo, attained an LDL cholesterol level of less than 100 mg per deciliter, and at least 90% of the patients who received SAR236553, as compared with 17% who received 80 mg of atorvastatin plus placebo, attained LDL cholesterol levels of less than 70 mg per deciliter (1.8 mmol per liter).
Conclusions:
In a randomized trial involving patients with primary hypercholesterolemia, adding SAR236553 to either 10 mg of atorvastatin or 80 mg of atorvastatin resulted in a significantly greater reduction in LDL cholesterol than that attained with 80 mg of atorvastatin alone.
Deel deze pagina met collega's en vrienden: