
PARAMOUNT: gunstige effecten van ARNI inhibitor bij Hartfalen pEF
Literatuur - Solomon SD et al, Lancet. 2012;380:1387-95
The angiotensin receptor neprilysin inhibitor LCZ696 in heart failure with preserved ejection fraction: a phase 2 double-blind randomised controlled trial.
Scott D Solomon, Michael Zile, Burkert Pieske, Adriaan Voors, Amil Shah, Elisabeth Kraigher-Krainer, Victor Shi, Toni Bransford, Madoka Takeuchi, Jianjian Gong, Martin Lefk owitz, Milton Packer, John J V McMurray, for the Prospective comparison of ARNI with ARB on Management Of heart failUre with preserved ejectioN fracTion (PARAMOUNT) Investigators
Lancet. 2012;380:1387-95. doi: 10.1016/S0140-6736(12)61227-6.
Achtergrond:
Hartfalen met behouden ejectiefractie (HFpEF) is verantwoordelijk voor ongeveer de helft van het aantal gevallen van hartfalen en gaat samen met een substantiële morbiditeit en mortaliteit [1-5]. Tot nu toe was er nog geen behandeling die de klinische uitkomsten bij deze aandoening verbeterde [6]. LCZ696 is de eerste angiotensin receptor neprisylin remmer die gelijktijdig het RAAS remt en het endogene natriuretisch peptidesysteem vergroot, wat beide gunstig kan zijn bij patiënten met hartfalen.De PARAMOUNT studie is een fase II studie in 301 patiënten uit 13 landen waarbij de effecten van LCZ696 en de ARB valsartan op de concentraties van natriuretische peptiden werden vergeleken in patiënten met hartfalen met behouden ejectiefractie.
Het natriuretisch peptide dat in deze studie werd onderzocht, NT-proBNP, is een marker van cardiale wandspanning; niveaus zijn verhoogd bij patiënten met hartfalen.
Resultaten:
- LCZ696 verminderde de niveaus van NT-proBNP met 23% in vergelijking met valsartan (p=0.005) (fig.1).
- LCZ696 verminderde ook vergroting van het linker atrium, een andere marker van nadelige uitkomsten bij hartfalen, en verbeterde de symptomen van hartfalen (fig. 2)
- LCZ696 werd goed verdragen met minder ernstige en overall adverse events dan valsartan
Conclusie:
LCZ696 heeft mogelijke gunstige effecten in patiënten met hartfalen met behouden ejectiefractie; nader onderzoek in deze patiënten wordt aanbevolen.
Figuur 1. (download als PPT)
NT-proBNP op 4, 12 en 36 weken in de LCZ696 en valsartan groepen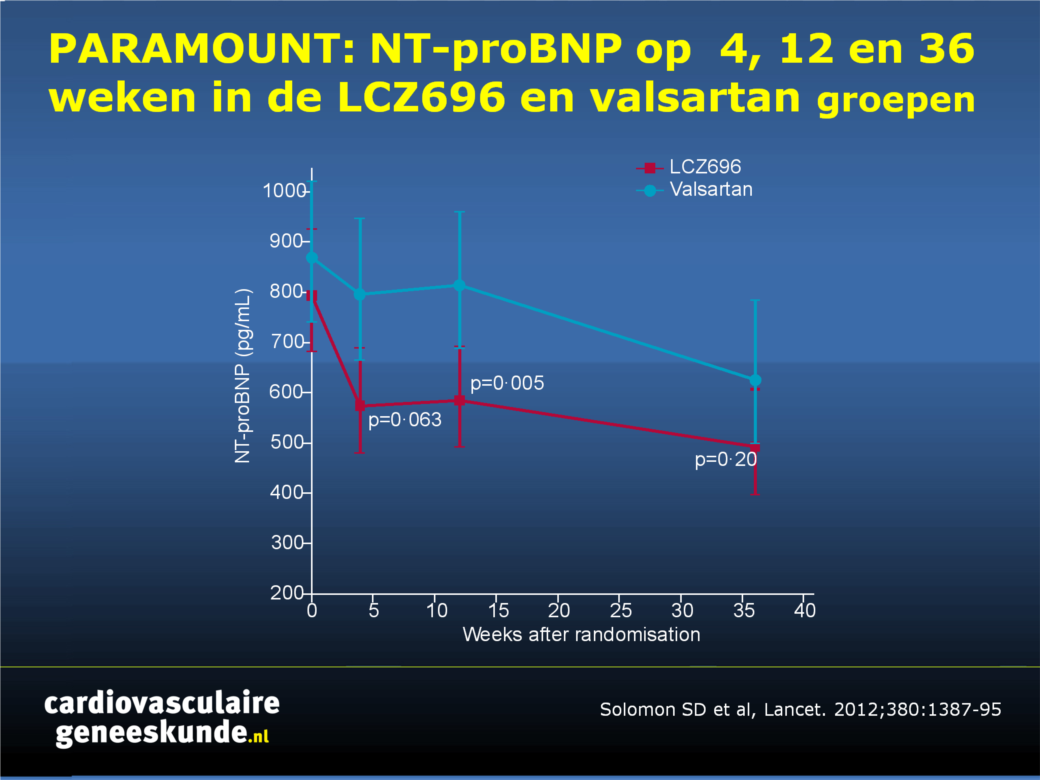
Figuur 2
Veranderingen in NYHA en klinisch samengestelde beoordeling met het percentage van patiënten die zijn verslechterd, onveranderd bleven, of verbeterden voor beide maten. NYHA = New York Heart Association.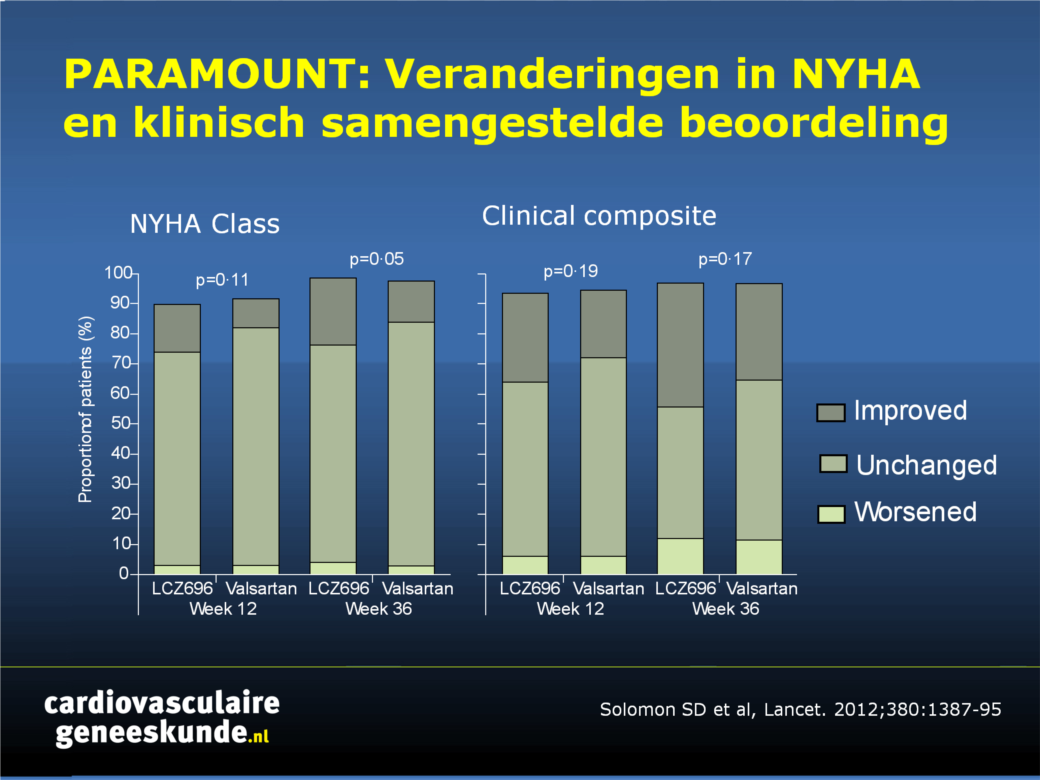
Referenties
1. Fonarow GC, Stough WG, Abraham WT, et al; OPTIMIZE-HF Investigators and Hospitals. Characteristics, treatments, and outcomes of patients with preserved systolic function hospitalized for heart failure: a report from the OPTIMIZE-HF Registry. J Am Coll Cardiol 2007; 50: 768–77.2. Lam CS, Donal E, Kraigher-Krainer E, Vasan RS. Epidemiology and clinical course of heart failure with preserved ejection fraction. Eur J Heart Fail 2011; 13: 18–28.
3. Bhatia RS, Tu JV, Lee DS, et al. Outcome of heart failure with preserved ejection fraction in a population-based study. N Engl J Med 2006; 355: 260–69.
4. Owan TE, Hodge DO, Herges RM, et al. Trends in prevalence and outcome of heart failure with preserved ejection fraction. N Engl J Med 2006; 355: 251–59.
5. Solomon SD, Anavekar N, Skali H, et al, Candesartan in Heart Failure Reduction in Mortality (CHARM) Investigators. Influence of ejection fraction on cardiovascular outcomes in a broad spectrum of heart failure patients. Circulation 2005; 112: 3738–44.
6. Aurigemma GP, Gaasch WH. Clinical practice. Diastolic heart failure. N Engl J Med 2004; 351: 1097–105.
Abstract
Background:
Heart failure with preserved ejection fraction is associated with substantial morbidity and mortality, but effective treatments are lacking. We assessed the efficacy and safety of LCZ696, a first-in-class angiotensin receptor neprilysin inhibitor (ARNI), in patients with this disorder.
Methods:
PARAMOUNT was a phase 2, randomised, parallel-group, double-blind multicentre trial in patients with New York Heart Association (NYHA) class II-III heart failure, left ventricular ejection fraction 45% or higher, and NT-proBNP greater than 400 pg/mL. Participants were randomly assigned (1:1) by central interactive voice response system to LCZ696 titrated to 200 mg twice daily or valsartan titrated to 160 mg twice daily, and treated for 36 weeks. Investigators and participants were masked to treatment assignment. The primary endpoint was change in NT-proBNP, a marker of left ventricular wall stress, from baseline to 12 weeks; analysis included all patients randomly assigned to treatment groups who had a baseline and at least one postbaseline assessment. This trial is registered at Clinicaltrials.gov, number NCT00887588.
Findings:
149 patients were randomly assigned to LCZ696 and 152 to valsartan; 134 in the LCZ696 group and 132 in the valsartan group were included in analysis of the primary endpoint. NT-proBNP was significantly reduced at 12 weeks in the LCZ696 group compared with the valsartan group (LCZ696: baseline, 783 pg/mL [95% CI 670-914], 12 weeks, 605 pg/mL [512-714]; valsartan: baseline, 862 pg/mL [733-1012], 12 weeks, 835 [710-981]; ratio LCZ696/valsartan, 0•77, 95% CI 0•64-0•92, p=0•005). LCZ696 was well tolerated with adverse effects similar to those of valsartan; 22 patients (15%) on LCZ696 and 30 (20%) on valsartan had one or more serious adverse event.
Interpretation:
In patients with heart failure with preserved ejection fraction, LCZ696 reduced NT-proBNP to a greater extent than did valsartan at 12 weeks and was well tolerated. Whether these effects would translate into improved outcomes needs to be tested prospectively.
Deel deze pagina met collega's en vrienden: