
PRoFESS: hartfrequentie en neurologische uitkomsten
Literatuur - Böhm M et al, Eur Heart J. 2012 Aug 26. [Epub ahead of print] - Eur Heart J. 2012 Aug 26. [Epub ahead of print
PRoFESS: Impact of resting heart rates on recurrent stroke, cardiovascular outcomes, disability and cognitive decline in 20.165 patients after ischemic stroke
Gepresenteerd door: Prof. Michael Böhm / Duitsland, ESC 2012; Clinical Trial & Registry Update I, 26 augustus 2012
Gepubliceerd: Böhm M, Cotton D, Foster L, et al. Impact of resting heart rate on mortality, disability and cognitive decline in patients after ischaemic stroke. .Eur Heart J. 2012 Aug 26. [Epub ahead of print]
Achtergrond
Recidiverende stroke is een veel voorkomende en invaliderende aandoening. Hoge hartfrequenties zijn geassocieerd met cardiovasculair risico. De effecten van de hartslag in rust op cardiovasculaire en neurologische uitkomsten na recidiverende stroke werden onderzocht in de hoog-risico populatie van de PRoFESS studie.20165 patiënten die na een ischemische stroke (gemiddelde leeftijd 66,1, SD 8,6 jaar) waren gerandomiseerd naar een van de armen van de PRoFESS studie werden gepooled, verdeeld in quintielen van de baseline hartslag en geanalyseerd op basis van cardiovasculaire en functionele uitkomsten na een beroerte. Recidief CVA en ernstige cardiovasculaire uitkomsten, zoals myocardinfarct, overlijden door cardiovasculaire oorzaak en noncardiovascular dood werden onderzocht. Vooraf gedefinieerde eindpunten waren invaliditeit na recidief CVA, gemeten met de gemodificeerde Rankin-schaal (MRS) en Barthel-index na 3 maanden, en cognitieve functie, gemeten met de Mini-Mental State Examination (MMSE) score op 4 weken na randomisatie en bij het voorlaatste bezoek .
Resultaten
- Patiënten in de twee hoogste kwintielen van hartslag (76-82 en> 82 slagen per minuut) hadden een hoger risico op totale sterfte (hazard ratio [HR] 1.42, 95% CI, 1,19-1,69 en [HR] 1.74, 95% BI, 1,48-2.06) ten opzichte van het laagste kwintiel.
- Soortgelijke resultaten werden waargenomen voor vasculaire sterfte en noncardiovascular sterfte. Risico's van recidief CVA (HR 1.11, 95% BI, 0,96-1,29) en MI waren niet significant verschillend bij patiënten met een hogere baseline hartslag.
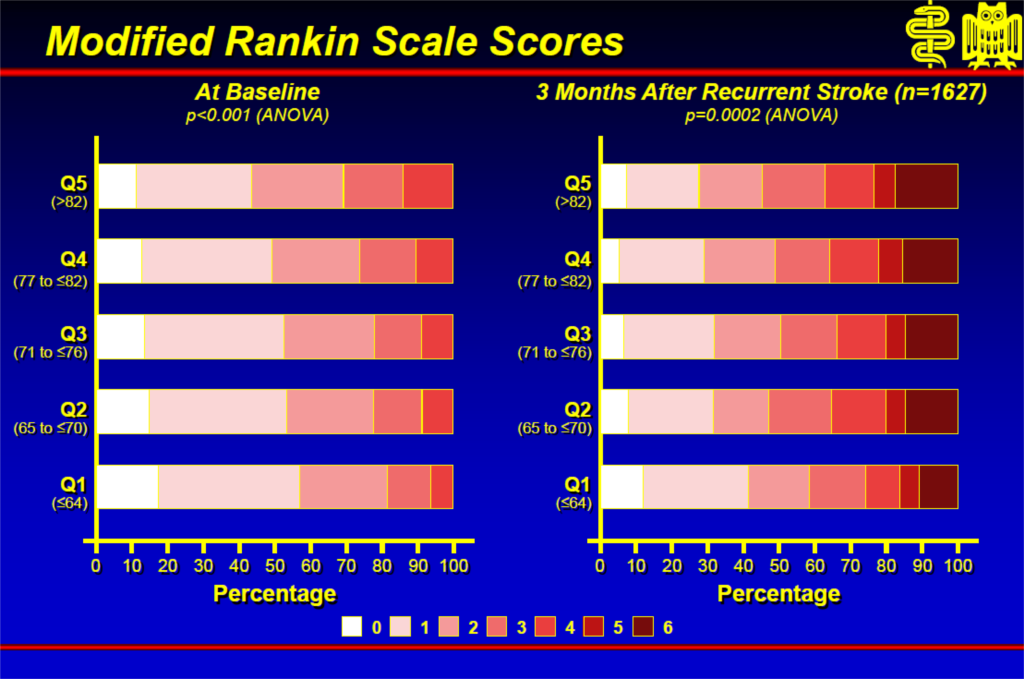
- Bij patiënten met een recidief CVA werd een associatie van een lagere hartslag met betere resultaten (Barthel) waargenomen bij alle hartslag groepen.
- Daarnaast was er een significante associatie van baseline hartslag tot significante cognitieve achteruitgang, gedefinieerd als een ≥ 2 punt verlaging in MMSE score tussen een maand en het voorlaatste bezoek.
Conclusie
Deze gegevens tonen aan dat de hartslag is geassocieerd met sterfte, maar niet met recidiverende stroke of MI bij patiënten na een stroke. Lage hartfrequenties zijn geassocieerd met betere neurologische functionele uitkomsten na een herseninfarct. Hogere hartfrequenties kunnen daarom in verband worden gebracht met grotere beroertes of verminderd herstel na een beroerte en zijn een algemene marker voor overleving bij deze patiënten.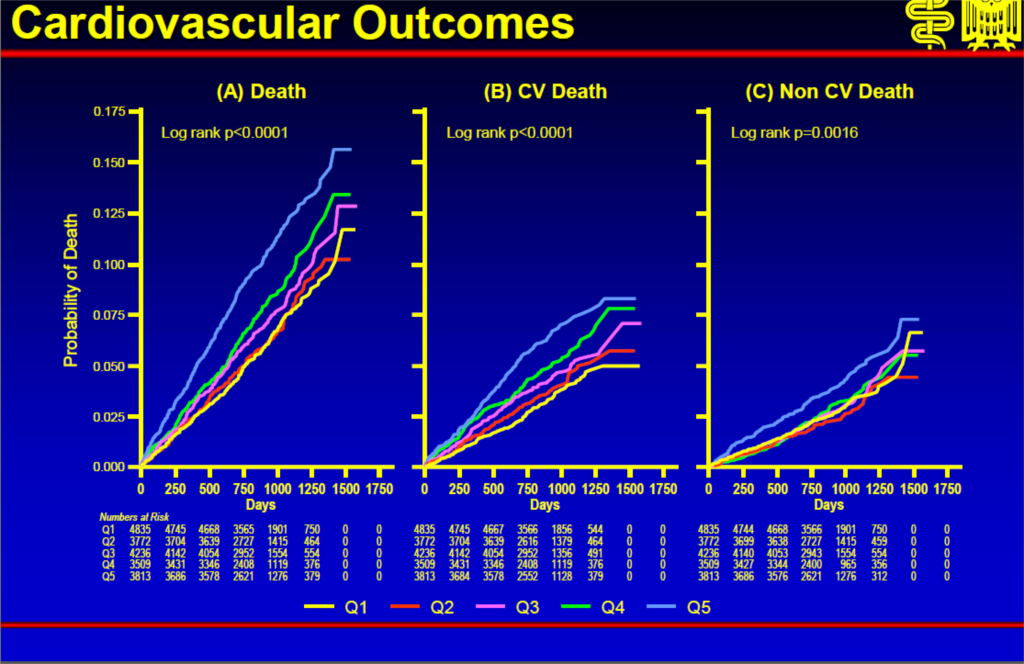
Abstract
AimsRecurrent stroke is a frequent and disabling event. A high heart rate is associated with cardiovascular outcomes. We investigated the effects of the resting heart rate on cardiovascular and neurological outcomes after recurrent stroke in the high-risk population of the PRoFESS study.
Methods and results
A total of 20 165 patients after ischaemic stroke (mean age 66.1, SD 8.6 years) assigned to the treatment arms of the PRoFESS trial were pooled divided by quintiles of the baseline heart rate and analysed according to cardiovascular and functional outcomes after stroke: recurrent stroke and major cardiovascular outcomes such as stroke, myocardial infarction, and worsening or new-onset heart failure as well as death from cardiovascular and non-cardiovascular causes. Pre-defined endpoints were disability after a recurrent stroke, assessed with the modified Rankin scale (mRS) and the Barthel index at 3 months, and cognitive function, assessed with the Mini-Mental State Examination (MMSE) score at 4 weeks after randomization and at the penultimate visit. Patients in the two highest quintiles of heart rate (77-82 and >82 b.p.m.) were at a higher risk for total death [hazard ratio (HR) 1.42, 95% CI 1.19-1.69 and HR 1.74, 95% CI 1.48-2.06, P < 0.0001] compared with the lowest quintile. Similar results were observed for vascular death [71-≤76 b.p.m., HR 1.39 (1.11-1.74), P < 0.0001] and non-vascular death [from >82 b.p.m., HR 1.66 (1.29-2.13), P = 0.0016]. Myocardial infarction (P = 0.7084) and recurrent stroke (P = 0.1379) were not significantly associated with the baseline heart rate. Hazard ratios were adjusted to multiple confounders including the baseline blood pressure. In the group of patients with a recurrent stroke, an association of a lower heart rate to better outcomes was measured with the Barthel index across all heart rate groups. In addition, there was a significant association of the baseline heart rate to the occurrence of significant cognitive decline according to an MMSE score ≤24 points at 1 month and at the penultimate visit or a decline of ≥2 points between these two time periods. Better independence score at a low heart rate were observed.
Deel deze pagina met collega's en vrienden: